6 Vaccine Myths

Ernest Board, Dr Edward Jenner performs first inoculation of 8-year old James Phipps (14 May 1796), painting from early 20th century │ source: Wikimedia Commons
Authors: Magdalena Kozela & Michał Zabdyr-Jamróz
Translation: Maja Nowak-Bończa
Originally published in Polish: 6 mitów na temat szczepionek, 16.11.2018
The benefits of using vaccinations are widely recognized by medical professionals [1], however, what is believed and propagated about them is increasingly less clear. The very fact that vaccinations are to be given to healthy people appears suspicious to laymen – as it is uncommon in medical procedures. In addition, they affect the entire population, including its more sensitive part, i.e. children. They are obligatory, which is interpreted as a form of coercion. Distrust of vaccination is fuelled more and more clearly by the so-called anti-vaccination movements that negate benefits of vaccination and seek to revise policies concerning it. The debate on the safety and obligation to vaccinate – conducted mainly using eristics: manipulated statistics and anecdotal evidence – contributed to the emergence of various „myths”, or rather grossly false beliefs. Below we present several of such myths, citing the latest scientific knowledge to refute them.
Myth 1: The spreading of non-communicable diseases results from the more frequent use of vaccination
The significant improvement of sanitary conditions, access to running water, refrigerators, introduction of preventive vaccinations and development of antibiotic therapy have significantly reduced the incidence and mortality from infectious diseases. At the same time, however, there has been an increase in incidence of other types of non-communicable diseases such as diabetes, obesity, allergies, cancers, various forms of autism and other mental disorders. These diseases have many causes and we do not fully understand their causes. They are referred to as “diseases of affluence” and civilization-related diseases, because the rapid, uncontrolled progress of civilization contributes to their development (e.g. traffic accidents). Many of these diseases are a fairly obvious result of the fact that we simply live longer, and that we are spared by some of the diseases that had so severely troubled our ancestors. We have eliminated a number of very deadly infectious diseases and now we are experiencing health problems that we once did not live long enough to encounter.
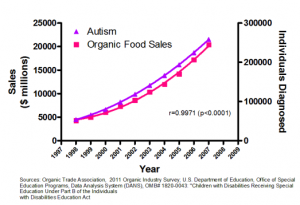
There is a clear correlation between the number of autism cases (triangles) and the sale of organic food (squares). Of course, this does not imply a causal relation. This is just one example of misleading correlations (from which one should not jump to conclusions) found on the website To tylko teoria│ source: ibid
Recognizing a given factor (in this case vaccines) as a cause of a specific disease is a long process and requires a lot of evidence. In epidemiology, a number of guidelines have been distinguished in this regard for a long time:
- A given factor would always have to precede the appearance of the disease. It is not enough that in some cases a given factor occurs simultaneously with the disease, because it can be a coincidence (e.g. it just so happens that autism spectrum symptoms are diagnosed at the age at which vaccines are usually administered).
- Studies of individual people in different groups (e.g. in different countries, in different age groups) indicate a strong, clear relationship. Analyzes of aggregated data and comparison of trends are insufficient because they could lead to the recognition of coincidence as a causal relation (see above).
- A given factor should not only be related statistically, but also through specific processes affecting the development of the disease (the so-called etiopathogenetic association). The mechanism by which a given vaccine affects the human body should be indicated, leading to, e.g. diabetes, cancer or developmental disorder.
- Removing the postulated cause (non-vaccination) should reduce the risk of a given disease.
The problem is that the arguments raised regarding the connection between vaccination and the occurrence of certain civilization diseases in the overwhelming majority do not meet these criteria. In addition, there is a whole series of reliable scientific studies clearly indicating the lack of any connection between vaccination administration and the incidence of these civilization diseases [2-4].
Myth 2: Vaccines cause autism

Retracted 1998 article by Andrew Wakefield et al. │ source: The Lancet
A good understanding of the nature of professional expert knowledge also implies the awareness that individual studies may be erroneous or misleading – whether due to methodological flaws or even fraud. Expert integrity demands caution in drawing hasty conclusions from any individual research. This applies in particular to those results that have shocking, sensational results, and which contradict already accumulated scientific knowledge. The process of making scientific research public in professional magazines contains mechanisms to ensure the accuracy of the final publication. This is called a peer-review process, in which anonymous experts receive an article from anonymous authors for evaluation and reject or allow it to be printed, usually indicating the need for corrections or clarifications. However, this process is flawed. It is particularly sensitive to fraud (reviewers usually assume the author’s good will and only try to help in the improvement of the text).
An example of fraudulent research is the famous Andrew Wakefield article from 1998 published in the prestigious scientific journal The Lancet [5]. It contained a description of the relationship between the occurrence of autism in children and the use of the ternary vaccine against measles, mumps and rubella (the so-called MMR vaccine). In 2004, a journalistic investigation by Brian Deer from The Sunday Times [6] showed that the results were false. Following further investigations in 2010, The Lancet retracted Wakefield’s article [7], and the author himself was banned from practicing in the United Kingdom. A number of practices that were incompatible with the researcher’s ethics were pointed out – from manipulation of the methodology through conflict of interest (participation in a company to develop replacement vaccines) to the abuse of the children participating in the study. Despite the scandal, the retraction of the publication and Wakefield’s disgrace, this article continues to be seen as an „evidence” of the alleged harmfulness of vaccines, being the main source of the false belief /fallacious reasoning that „vaccines cause autism”.
Myth 3: Vaccination is not mandatory in other countries, so Poland should not make it compulsory
Legal regulations regarding the obligation to vaccinate differ significantly between European and world countries. There are countries where vaccinations are not compulsory while the vaccination rates (i.e. the percentage of vaccinated populations) reach 95-99% (Scandinavian countries). There are also countries (such as France) where, despite the legal obligation, the percentage of vaccinated individuals is well below the threshold of what is known as population immunity. Population (or „herd”) immunity is a situation in which there is no infection among those who cannot be vaccinated, because those who could infect them have been vaccinated and do not get sick.
Animation (prepared by a redditer) illustrating the „herd immunity” phenomena. Dots in various colors mark the infected (black); not vaccinated (blue); and vaccinated (yellow).
It is worth noting that there has been an increase in the threat of a measles epidemic, which has been observed in recent years along with the decreasing rates of vaccination throughout Europe. To stop the spread of measles, it is necessary to maintain a level of not less than 95%. At this level of vaccination, a susceptible person has very little chance of contacting a sick person. In September 2018, the European Center for Disease Prevention and Control (ECDC) published a report on measles incidence in the previous year (from August 2017 to July 2018), which shows that in European countries this status has not been maintained. More than 14,000 measles cases have been reported in EU countries. The highest incidence rates (number of cases per 1 million inhabitants) were recorded in Greece (299.4), Romania (78.2), Slovakia (65.5), Italy (47.4) and France (41.7). There have been 37 deaths due to measles, including 25 in Romania where there is no legal obligation to vaccinate. The European Commission has also expressed concern about the rapid increase in measles in Europe.
Elvis Presley participated in vaccination promotion campaigns | circa 1956
The goal of health policy regarding vaccination is to achieve population immunity. The legal obligation is one of the instruments employed to reach this goal, and it is often a key instrument. Of course, it is not universally used, nor is it 100% effective. But this should not be an argument for depriving Polish society of one of the most effective tools for ensuring health safety for its most vulnerable members. The fact that in some countries the mandatory vaccination has not led to the most desirable level of immunity does not mean that this obligation was not needed. This certainly does not mean that it would be better without this mandate. It is quite likely that it would be even worse without it.
The myth of comparing yourself to other countries has an additional element: the allegation that mandatory vaccinations violate a person’s right to respect for private life contained in the European Convention on Human Rights. This position is completely untrue – it is based on blatantly false references to actual provisions of the European Court of Human Rights (more on the issue of these manipulations can be found in the analysis of the justification of the bill concerning the elimination of mandatory vaccination, which was rejected by the Polish Senate).
Although population immunity still works in Poland, even with mandatory vaccination, the population-securitability indexes cannot be maintained. Lifting this obligation can only make things worse. Especially that it is accompanied by harmful misinformation instead of sensible health policy (e.g. education about the risk of infectious diseases and vaccination safety).
Myth 4: Vaccinations are harmful to premature babies
Polish Compulsory Preventive Vaccination Program indicates that vaccination of prematurely born children should take place according to their chronological age, i.e. from birth. This is due to the fact that premature babies in particular require artificial immunization due to their underdeveloped immune system. Premature babies have fewer antibodies passed from the mother through the placenta and less developed immunity at the cellular level, which means that they are more likely to have infectious diseases than term-born children. A number of studies confirm that premature babies have a higher risk of developing diseases such as invasive pneumococcal disease and whooping cough, which can be fatal. It has been confirmed that vaccination against these diseases is effective and reduces the risk of falling ill both in premature babies and in babies born at term [8-10]. It has also been shown that prematurity is a factor which increases the likelihood of post-influenza complications, and influenza vaccination is an effective method for avoiding these complications [10].
https://www.youtube.com/watch?v=EZ7lL7Pzcws
Myth 5: Young children are overburdened by vaccines

A child in India receives an oral polio vaccine │ source: wikimedia commons
On the first day after birth, the respiratory system, digestive system and baby’s skin are colonized by a huge number of microorganisms. From this moment, the child’s immune system begins to learn how to fight external threats, which allows him or her to survive in the future. It is estimated that there are about 1,000 bacteria per 1 cm2 of healthy skin, and about 100 million in 1 g of human saliva. Considering how young children function – especially in a peer group, on a playground, in a nursery or kindergarten – their exposure to huge amounts of antigens is perfectly normal. Meanwhile, the average vaccine for a small child contains from a few to a dozen antigens.
Research results published in March 2018 in the scientific journal JAMA (Journal of Americal Medical Association) indicate that the administration of many vaccines in the first two years of a child’s life does not have a negative impact on the immune system. The authors counted the total number of antigens in vaccines received by the examined children during their first 23 months of life, then compared the number of antigens administered between children aged 2-4 years who developed infections (against which vaccines do not protect), and randomly selected children of this age who did not get sick. The cumulative number of antigens did not differ significantly between these groups of children. Therefore, no relation between vaccinations and subsequent development of other infections was found [11].
Myth 6: Anti-vaccination campaigns are based on extensive knowledge
The information provided by anti-vaccination organizations has a simple, clear message. They often use individual cases to illustrate negative phenomena (anecdotal evidence) and evoke strong emotions. They attract attention and are understandable to the average person. Most often, however, this is not information from medical professionals, but only self-taught amateurs. These people do not know the broader context of the issue and seek only the knowledge that is consistent with their previous views. The simplicity and unambiguity of the message results from this bias, its incomplete understanding or evident instrumentalization of cherry-picked data.
Sound scientific knowledge from reliable sources is rarely so explicit or sensational. It is the result of the synthesis of numerous studies carried out by numerous researchers over the span of many years. These studies are tedious, carried out according to methods that are designed to suppress bias and emotional or financial motivations. Preparing reliable information on the results of these studies for laymen (including experts from other fields) requires an effort comparable to translating from a foreign language. It requires a good mastery of the discipline’s expert jargon and the ability to translate it into natural language. Many terms of scientific language – sounding identical to words commonly used in colloquial speech – have a specific technical meaning, sometimes clearly different from that of everyday language. All this means that many errors, distortions and prejudices may creep in to the interpretation of even true scientific knowledge.
Interesting research results have recently been published that assess the relationship between knowledge and opinions on autism spectrum conditions and vaccination policies. It showed the occurrence of a psychological phenomenon called the Dunning-Kruger effect. This occurs when unskilled people in some area overestimate their skills in the given area, while highly qualified people sometimes show excessive caution. Exactly such a phenomenon was observed in relation to laymen talking about the relationship between vaccinations and autism spectrum disorders. Over-confidence has also been shown to have important implications for vaccine policy. People who believe that they know more than medical professionals are less supportive of pro-vaccine policies and support the participation of non-experts in the development of vaccination regulations [12].
* * *
In Poland, the discussion about the legitimacy of using vaccinations, their safety and compulsory nature comes back regularly. At the same time, we have seen a dramatic increase in the number of people avoiding compulsory vaccinations in recent years (over 30,000 refusals in 2017). Nevertheless, the August 2017 study conducted by CBOS indicates that the majority of respondents do not at all expect to abandon the mandatory vaccination of children. The vast majority of respondents (80%) appreciate the positive effects of vaccinations and want to maintain this obligation. Only 12% of respondents believe that no vaccinations should be compulsory and that only parents should decide about vaccinating or not vaccinating a child. On the other hand, this study showed a lack of parents’ knowledge about vaccination. Interestingly, Poles – especially those with children – expect solutions to be directed, above all, at limiting the contact of unvaccinated children with vaccinated ones rather than using financial penalties for parents who have avoided vaccinating their children [13].
In conclusion, it should be emphasized that, according to current medical knowledge, vaccinations are the most effective method of protection against infectious diseases. There are no credible scientific studies that would indicate that massive use of vaccinations is causally associated with non-communicable diseases. Protective vaccinations are a medical procedure, the use of which is of great importance not only for the vaccinated, but also for the weakest members of society (for people who cannot be vaccinated). Among other things, for this reason, the decision to vaccinate should not be left only to those who are not competent to properly assess current medical knowledge. Anti-vaccine activists make up a small proportion of the population and are most often not medical professionals. Their message is not confirmed by scientific research. Fortunately, most Poles understand the need and benefits of preventive vaccinations. Unfortunately, the lack of knowledge and understanding of the subject leads to the acceptance of myths about vaccines, resulting not only in evasion of vaccination, but also unwittingly striving to broadly weaken the health safety of the weakest – including their own, unvaccinated children.
Contact with authors: Magdalena Kozela, Michał Zabdyr-Jamróz
Public Health Blog, ed. M. Zabdyr-Jamróz, Instytute of Public Health JU MC, Kraków: 11 February 2020
Sources:
- Matkowska-Kocjan A., Szenborn L. 2010. Bezpieczeństwo szczepień w świetle najnowszej wiedzy medycznej. Przewodnik Lekarza, 13(5).
- Morgan E., Halliday S.R., Campbell G.R., Cardwell C.R., Patterson C.C. 2016. Vaccinations and childhood type 1 diabetes mellitus: a meta-analysis of observational studies. Diabetologia, 59(2): 237-43.
- Madsen K.M., Hviid A., Vestergaard M., Schendel D., Wohlfahrt J., Thorsen P., Olsen J., Melbye M. 2002. A population-based study of measles, mumps, and rubella vaccination and autism. N Engl J Med., 347(19): 1477-82.
- El-Zein M., Conus F., Benedetti A., Menzies D., Parent M.E., Rousseau M.C. 2017. Association Between Bacillus Calmette-Guérin Vaccination and Childhood Asthma in the Quebec Birth Cohort on Immunity and Health. Am J Epidemiol., 1; 186(3): 344-355.
- Wakefield A. J. et al. 1998. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children, The Lancet, 351(9103): 637-641.
- Deer B. 2011. How the case against the MMR vaccine was fixed, British Medical Journal, 342, art. nr c5347.
- The Lancet 2010. Retraction: Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children, The Lancet, 375(9713): 445.
- Riise Ø.R., Laake I., Vestrheim D., Winje B.A., Moster D., Storsæter J. 2018. Preterm Children Have Higher Risk Than Full-term Children of Invasive Pneumococcal Disease During the First 2 Years of Life. Pediatr Infect Dis J., 37(7): e195-e200.
- Riise Ø.R., Laake I., Vestrheim D., Flem E., Moster D., Riise Bergsaker M.A., Storsæter 2017. Risk of Pertussis in Relation to Degree of Prematurity in Children Less Than 2 Years of Age. J.Pediatr Infect Dis J., 36(5): e151-e156.
- Gill PJ, Ashdown HF, Wang K, Heneghan C, Roberts NW, Harnden A, Mallett S. 2015. Identification of children at risk of influenza-related complications in primary and ambulatory care: a systematic review and meta-analysis. Lancet Respir Med. Feb; 3(2): 139-149.
- Glanz J.M., Newcomer S.R., Daley M.F., et al. 2018. Association Between Estimated Cumulative Vaccine Antigen Exposure Through the First 23 Months of Life and Non–Vaccine-Targeted Infections From 24 Through 47 Months of Age. JAMA. 319(9): 906–913.
- Motta M., Callaghan T., Sylvester S. 2018. Knowing less but presuming more: Dunning-Kruger effects and the endorsement of anti-vaccine policy attitudes. Soc Sci Med. Aug 211: 274-281.
- CBOS 2017. Komunikat z badań, nr 100/2017, Warszawa.
 FACEBOOK
FACEBOOK INSTAGRAM
INSTAGRAM X
X LINKEDIN
LINKEDIN YOUTUBE
YOUTUBE